Friday, April 20, 2012
Wednesday, April 18, 2012
Ian McColl - Pink and Purple
Two cases, one pink and one purple.
Case 1 A young 34 years old female who noted this growing on her forearm for about 6 weeks.




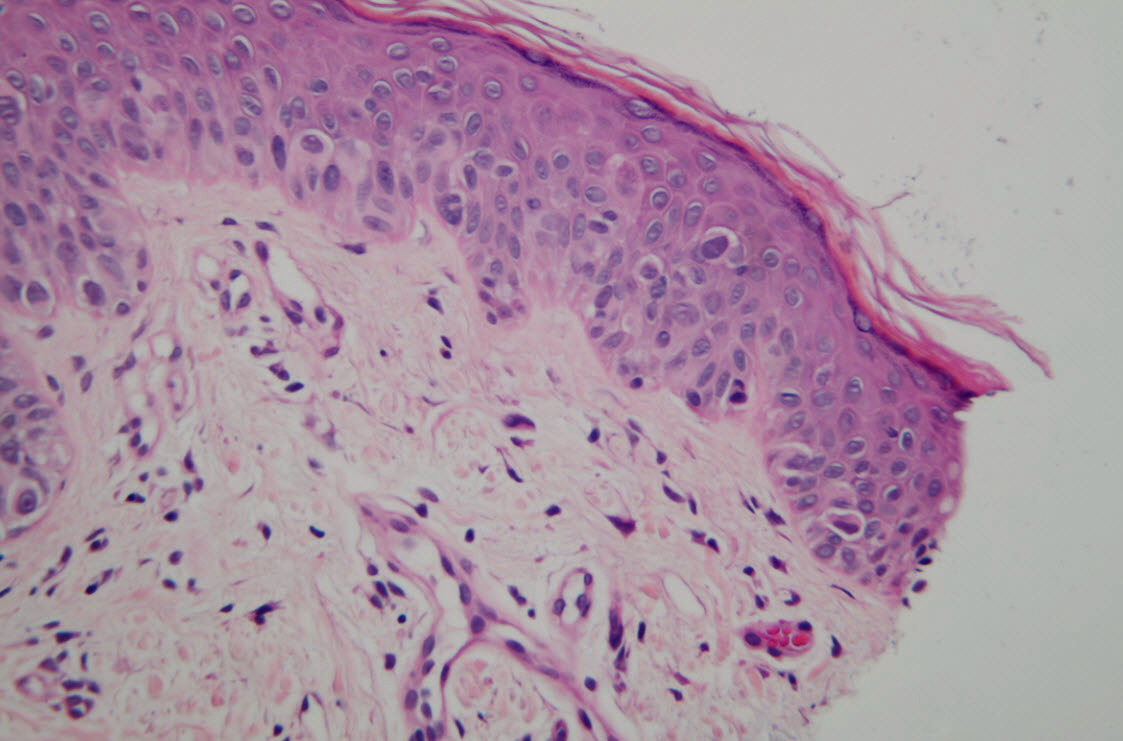
Case 1 Histology. This I think is a tough one.





Case 2 A male in his 60s with several month's history of this lesion on his lower leg. No history of a pre existing lesion. It was not itchy. Nothing had been applied to it. No similar lesions elsewhere.I was impressed by the colour.




This is the histology for Case 2. Punch biopsies were taken of the pink and the purple areas. First 3 are from the pink area and the last three from the darker purple area.
Case 2 Pink Area



Case 2 Dark area


 Dr Jeff Keir said...
Dr Jeff Keir said...
Case 1 non-pimented raised lesion. Vessels as dots: amelanotic spitz/ compound/dermal nevus / melanoma in ddx. Is the yellowish background significant? Don't know. Needs bx, let the pathologist sort it!
Case 2: a very florid LPLK in a borad solar lentigo seb k. Very few things look like this - and there are centred vessels and brown/yellow clods (keratin plugs) t the edge supporting the LPLK in seb k dx.
Dr Ian McColl said...
I thought the purple was very like lichen planus but it was a solitary non itchy lesion. Lichen planus on the legs can look like this but that was not the histology.
Dr Ian McColl said...
I have put up the histology of case 2. If lichen planus there should have been a florid lymphocytic infiltrate eating away at the basement membrane zone but it is much milder.
Dr Ian McColl said...
Nothing too worrying about Case 2 It was reported as a lichenoid keratosis but there is epidermal acanthosis and hyperkeratosis and I am sure Jeff was correct that this is a lichenoid reaction to a Seb K. I will put up the histo to case 1.( Been occupied with a medical student this afternoon!)
Dr Ian McColl said...
As a hint for the pathology it is malignant and there are some atypical melanocytes at the DEJ in some areas but the main feature are all the spindled cells in the dermis. What is it?
5:29 PM
Dr Con Pappas said...
Spindle cells would equal desmoplastic MM with those atypical melanocytes Ian. Then you have the DD of all the spindle cell tumours which you need immunohistochemistry to sort out.
Dr Ian McColl said...
Correct. Desmoplastic melanoma 2.6 mm thick. She had sentinel lymph node examination done which was clear. She is a reliable witness. This thing grew very quickly. They really are featureless. You have no option but to excision biopsy it straight away if you get a pink nodule and let the pathologist decide.
Graeme Siggs said...
Straight out of DermNetNZ:
Desmoplastic melanomas may have a slightly better prognosis compared to other subtypes of the same thickness.
A study of 1129 desmoplastic melanoma patients in the United States (1992-2007) reported a 5-year specific survival rate of 85% and 10-year survival of 80%. Older age, anatomic site of the head and neck and tumour thickness >2 mm, ulceration, lymph node involvement and non-receipt of surgery were associated with lower survival. A second study of 1,735 desmoplastic melanoma patients, also in the United States (1988-2006), reported overall survival at 5 years to be 65% and that wide local excision was associated with increased survival. Traditional prognostic factors such as Breslow thickness, nodal positivity, and ulceration did not predict survival in this group of patients.
The SMU reports better survival than this though.
See this abstract:
http://jco.ascopubs.org/content/24/8/e12.full
In SMU patients with localized disease, the 5-year survival rate in 280 DM patients (90%)was significantly higher than in all 7,767 cutaneous melanoma patients incorporated into the American Joint Cancer Committee on Cancer staging database (82%),despite the fact that median tumor thickness in the former group was considerably greater than in the latter (2.5 mm v 1.6 mm, respectively) group.
Case 1 A young 34 years old female who noted this growing on her forearm for about 6 weeks.




Case 1 Histology. This I think is a tough one.




Case 2 A male in his 60s with several month's history of this lesion on his lower leg. No history of a pre existing lesion. It was not itchy. Nothing had been applied to it. No similar lesions elsewhere.I was impressed by the colour.




Case 2 Pink Area



Case 2 Dark area



Case 1 non-pimented raised lesion. Vessels as dots: amelanotic spitz/ compound/dermal nevus / melanoma in ddx. Is the yellowish background significant? Don't know. Needs bx, let the pathologist sort it!
Case 2: a very florid LPLK in a borad solar lentigo seb k. Very few things look like this - and there are centred vessels and brown/yellow clods (keratin plugs) t the edge supporting the LPLK in seb k dx.
Dr Ian McColl said...
I thought the purple was very like lichen planus but it was a solitary non itchy lesion. Lichen planus on the legs can look like this but that was not the histology.
Dr Ian McColl said...
I have put up the histology of case 2. If lichen planus there should have been a florid lymphocytic infiltrate eating away at the basement membrane zone but it is much milder.
Dr Ian McColl said...
Nothing too worrying about Case 2 It was reported as a lichenoid keratosis but there is epidermal acanthosis and hyperkeratosis and I am sure Jeff was correct that this is a lichenoid reaction to a Seb K. I will put up the histo to case 1.( Been occupied with a medical student this afternoon!)
Dr Ian McColl said...
As a hint for the pathology it is malignant and there are some atypical melanocytes at the DEJ in some areas but the main feature are all the spindled cells in the dermis. What is it?
5:29 PM
Dr Con Pappas said...
Spindle cells would equal desmoplastic MM with those atypical melanocytes Ian. Then you have the DD of all the spindle cell tumours which you need immunohistochemistry to sort out.
Dr Ian McColl said...
Correct. Desmoplastic melanoma 2.6 mm thick. She had sentinel lymph node examination done which was clear. She is a reliable witness. This thing grew very quickly. They really are featureless. You have no option but to excision biopsy it straight away if you get a pink nodule and let the pathologist decide.
Graeme Siggs said...
Straight out of DermNetNZ:
Desmoplastic melanomas may have a slightly better prognosis compared to other subtypes of the same thickness.
A study of 1129 desmoplastic melanoma patients in the United States (1992-2007) reported a 5-year specific survival rate of 85% and 10-year survival of 80%. Older age, anatomic site of the head and neck and tumour thickness >2 mm, ulceration, lymph node involvement and non-receipt of surgery were associated with lower survival. A second study of 1,735 desmoplastic melanoma patients, also in the United States (1988-2006), reported overall survival at 5 years to be 65% and that wide local excision was associated with increased survival. Traditional prognostic factors such as Breslow thickness, nodal positivity, and ulceration did not predict survival in this group of patients.
The SMU reports better survival than this though.
See this abstract:
http://jco.ascopubs.org/content/24/8/e12.full
In SMU patients with localized disease, the 5-year survival rate in 280 DM patients (90%)was significantly higher than in all 7,767 cutaneous melanoma patients incorporated into the American Joint Cancer Committee on Cancer staging database (82%),despite the fact that median tumor thickness in the former group was considerably greater than in the latter (2.5 mm v 1.6 mm, respectively) group.
Subscribe to:
Posts (Atom)